There are several senses in which the health of women
and girls can be considered as the basic indicators
for the health of a society. Precisely because of
gender discrimination, the health conditions of females
generally tend to lag behind those of males, and therefore
absolute improvement in these conditions is a reasonable
indicator that the overall health conditions of that
society are also getting better.
In the past two decades, India had the third fastest
growing economy in the Asian region (after China and
Vietnam) and it is generally perceived even in a period
of continuing global crisis, as an emerging economic
powerhouse. Table 1 presents India’s growth performance
in the past two decades in relation to three other
Asian countries. Vietnam grew slightly faster than
India but still has slightly lower per capita income.
Sri Lanka is richer on average but has growth more
slowly, while Bangladesh is still clearly a low income
country, where per capita income has increased, though
more slowly than these other countries.
Table
1: |
|
Annual
per capita income change 1990-2010 (%) |
National
Income per capita, US $ in 2010
|
Bangladesh |
3.49 |
700
|
India |
4.90 |
1340
|
Sri
Lanka |
4.22 |
2240
|
Vietnam |
5.95 |
1110
|
Table
1 >>
Click
to Enlarge
To what extent was this period of economic expansion
in India reflected in better health outcomes for women
and girls? To examine this, we consider two crucial
health indicators: the female Infant Mortality Rate
(IMR or number of deaths per 1000 children below one
year) and the Maternal Mortality Ratio (MMR or number
of childbirth-related deaths per 100,000 live births).
Chart
1 >> Click
to Enlarge
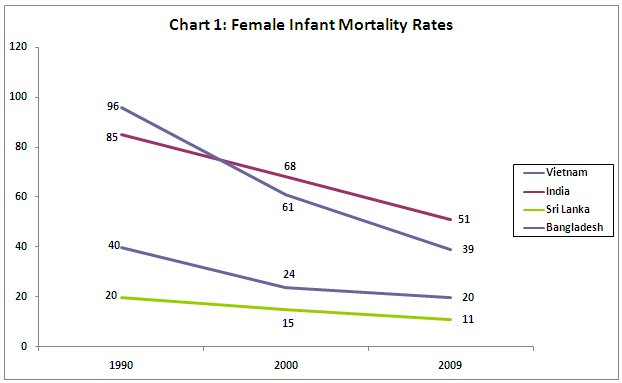
Chart
1 shows that in terms of female infant mortality rates,
India is by far the worst performer in this group,
with the slowest rate of decline. Even Bangladesh,
which is much poorer and has slower national income
growth, managed to bring the female IMR down faster.
And the Indian rate is more than two and a half times
that of Vietnam, which has a lower per capita income.
Chart
2 >>
Click
to Enlarge
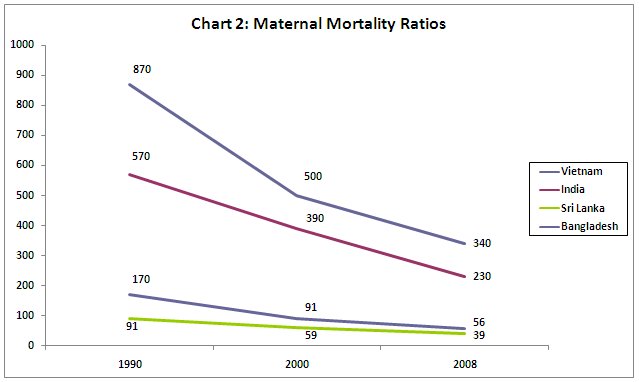
The evidence on maternal mortality is equally disturbing.
India and Bangladesh both have very high rates, many
multiples of those in Sri Lanka and Vietnam. But even
here, the rate of reduction of this ratio has been
marginally faster in Bangladesh.
Of course India is also very regionally diverse, with
some states like Kerala showing excellent health outcomes
for women, similar to those in Vietnam. And three
states have also shown much improved health indicators
in the past two decades: Tamil Nadu, West Bengal and
Maharashtra. But the bulk of the country still shows
generally appalling levels of female IMR and MMR.
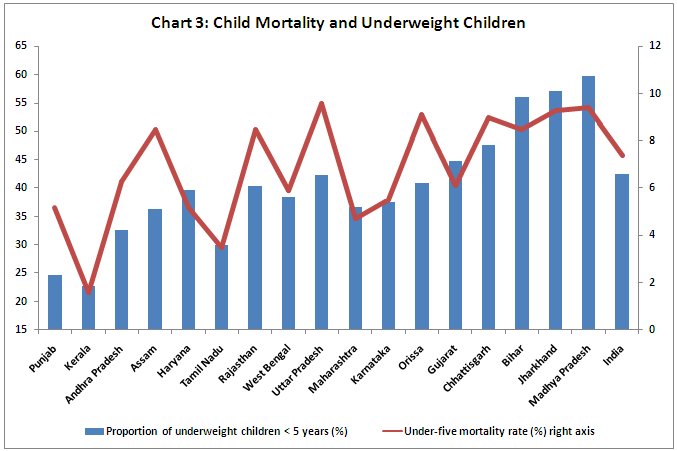
One important reason for high infant and child mortality
is under-nutrition, which has actually worsened in
recent times according to indicators like calorie
consumption. Rising prices of food are making this
problem worse as women and girls in poor households
take the brunt of food scarcity. Chart 3 shows how
closely the rate of child mortality tracks the proportion
of underweight children across Indian states.
Chart
3 >>
Click
to Enlarge
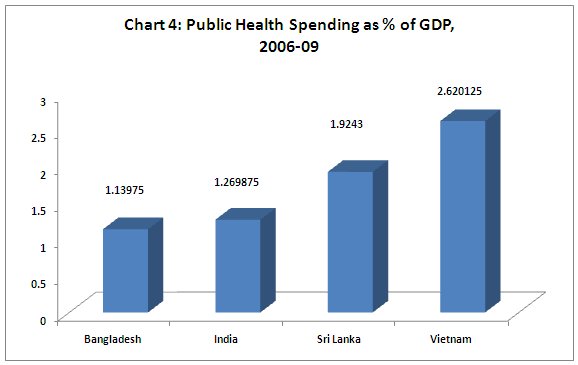
Nutrition is important, but it is not the only concern.
To deliver better health outcomes, public expenditure
on health service delivery is absolutely essential,
and this is especially important for women and girl
children. Here again, India fares badly. Public spending
on health (as Chart 4 shows) is a minuscule amount
in relation to GDP, and around two-third of health
expenditure is out-of-pocket payment by households.
This is indeed an important reason for families falling
into poverty or remaining destitute, and gender biases
reinforce the relative denial of health care to women
and girls in such conditions.
Chart
4 >>
Click
to Enlarge
Even in absolute per capita terms, public health spending
in India is around half that in Vietnam, which is
a country with lower per capita income. And it is
just above one-third of the level in Sri Lanka. It
is true that Bangladesh show a much lower level, but
then Bangladesh also has a much lower per capita income.
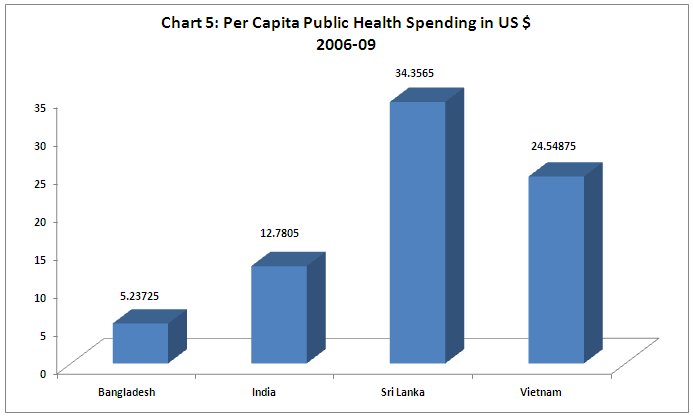
Chart
5 >>
Click
to Enlarge
So it is no wonder that other indicators of health
service delivery also appear quite inadequate with
respect to the other countries. Chart 6 shows that
less than half of births are attended by skilled personnel,
whereas in Vietnam it is near universal and it is
close to that in Sri Lanka. The low proportion here
suggests one important reason for the high maternal
mortality ratios in India and Bangladesh.
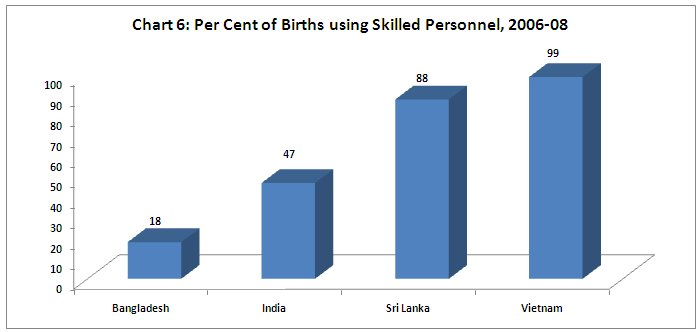
Chart
6 >>
Click
to Enlarge
Similarly, immunisation coverage is a necessary element
in ensuring child health. Full measles coverage within
the first year of life is often taken as a proxy for
the extent of immunisation in general, and in this
case India fares worst among this set of four countries.
Even Bangladesh has much higher immunisation rates.
In some parts of the country, immunisation rates have
barely improved. Small wonder then, that infant mortality
rates has come down more slowly in India than in these
other countries.
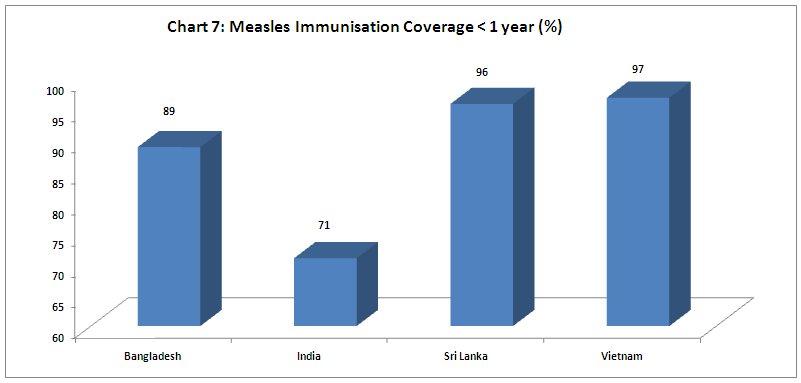
Chart
7 >>
Click
to Enlarge
Another
major aspect of ensuring adequate health conditions
is the provision of improved sanitation for everyone.
This is one of the weakest aspects, along with nutrition:
around 70 per cent of the population do not have access
to improved toilets. Remarkably, this does not even
appear as a major policy goal for the government,
which does not appear to see the urgency in this matter,
or the wider health effects, quite apart from the
loss of dignity to citizens that comes from forced
open defaecation.
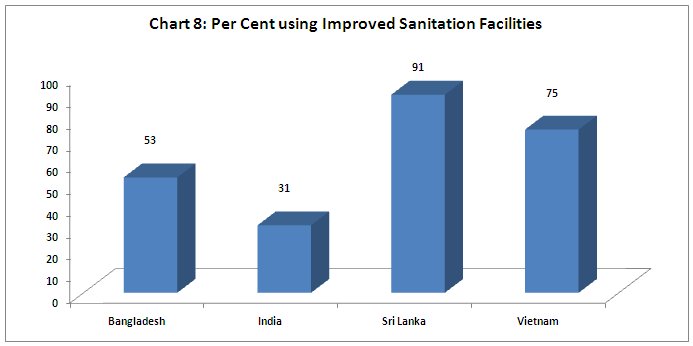
Chart
8 >>
Click
to Enlarge
All
of these factors are crucially determined by government
policy. Despite much publicly expressed concern on
all these issues, the Government of India has simply
not put its money where its mouth is. Public spending
as a share of GDP has not increased, and per capita
spending on some essential activities like immunisation
and primary health centres has actually gone down.
Instead, the government has sought to provide essential
health services on the cheap, using the underpaid
labour of local women working for much less than the
minimum wage, not properly trained regular public
employees with adequate facilities.
The apparently growing divide between economic growth
and women’s health outcomes in countries like India
is not inevitable: the experience of other Asian countries
shows that a more positive synergy can be created,
with health spending not just valued for its own sake,
but as an essential element in an overall macroeconomic
and growth framework oriented to better conditions
of human life rather than just GDP expansion.
*
This article was originally published in the Business
Line on November 28, 2011.
