The Unfulfilled Potential of the ICDS
This
year marks the 30th anniversary of the Integrated Child Development
Scheme, or ICDS, which was initiated in October 1975 in response
to the evident problems of persistent hunger and malnutrition especially
among children.
Since
then, the ICDS has grown to become the world’s largest early child
development programme. The coverage of the Scheme has expanded rapidly,
especially in recent years. From an initial 33 blocks in 1975, the
programme covered an estimated 6,500 blocks by 2004. There are almost
600,000 anganwadi workers and an almost equal number of anganwadi
helpers providing services to beneficiaries throughout the country.
According to the government, the programme currently reaches 33.2
million children and 6.2 million pregnant and lactating women.
Officially, the objectives of the Scheme are:
-
to improve the nutritional and health status of children in the age group 0-6 years
-
to lay the foundation for proper psychological, physical and social development of the child
-
to reduce the incidence of mortality, morbidity, malnutrition and school drop out
-
to achieve effective coordinated policy and its implementation amongst the various departments to promote child development
-
to enhance the capability of the mother to look after the normal health and nutritional needs of the child through proper nutrition and health education
Accordingly,
the ICDS involves the setting up of anganwadi centres, each of which
is intended to cater to a population of around 1,000 in rural and
urban areas and to around 700 in tribal areas. The anganwadi worker
and helper, who are the basic functionaries of the ICDS, run the
anganwadi centre and implement the Scheme in coordination with the
functionaries of the health, education, rural development and other
departments. They are called ‘social workers’ and are paid an honorarium
of Rs. 1,000 per month for the worker and Rs. 500/- for the helper.
However, the supervisors and other higher officials are government
employees.
The anganwadis are meant to provide the following services:
-
supplementary nutrition to children below 6 years of age, and nursing and pregnant mothers from low income families
-
nutrition and health education to all women in the age group of 15- 45 years
-
immunisation of all children less than 6 years of age and immunisation against tetanus for all the expectant mothers
-
health check up, which includes antenatal care of expectant mothers, postnatal care of nursing mothers, care of newborn babies and care of all children under 6 years of age
-
referral of serious cases of malnutrition or illness to hospitals, upgraded PHCs/ Community Health Services or district hospitals
-
non-formal preschool education to children of 3-5 years of age.
By many accounts, thus far the scheme has been a success. Most of the studies conducted on the functioning of the ICDS Scheme have recognised its positive role in the reduction of infant mortality rate, in improving immunisation rates, in increasing the school enrolment and reducing the school drop out rates. The most important impact of the Scheme is clearly reflected in significant declines in the levels of severely malnourished and moderately malnourished children and Infant Mortality Rate in the country. The percentage of children suffering from severely malnutrition declined from 15.3 per cent during 1976-78 to 8.7 per cent during 1988-90. Infant Mortality Rates declined from 94 per 1000 live births in 1981 to 73 in 1994.
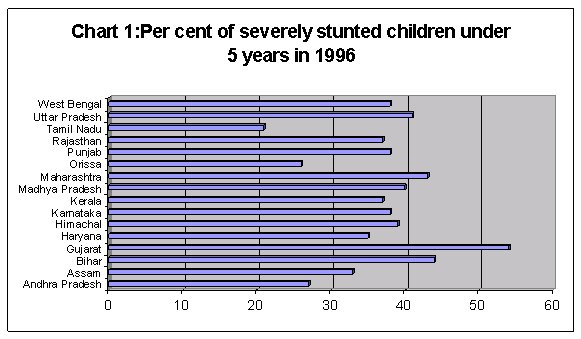
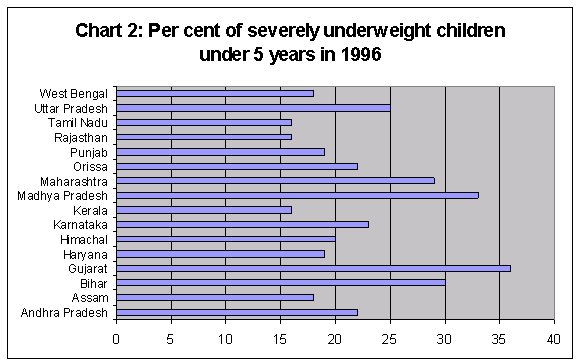
Nevertheless, it is also clear that for a scheme that has been in operation for three decades, the benefits are still far too limited, and maternal and child health and nutrition are still areas of major concern for policy. Even today, around one third of Indian children – and more than half in rural areas - are born with low birth weight. Charts 1 and 2 indicate the extent of severe stunting and severe under-nutrition among young children in the major states, both of which are still unacceptably high. It is noteworthy that these indicators are particularly bad in some ostensibly more ''developed'' and relatively high-income states, such as Gujarat, Maharashtra and Karnataka.
The high incidence of premature births, low birth weight and neonatal and infant mortality can be attributed to poor nutritional conditions of the mothers. The majority of women still do not get proper nutrition and health care during their pregnancy. In some areas, 60-75 per cent of pregnant women receive no antenatal care at all. More than 85 per cent of women in rural areas and 95 per cent in the remote areas give birth at home. Only 42 per cent of women in the country have access to safe delivery facilities.
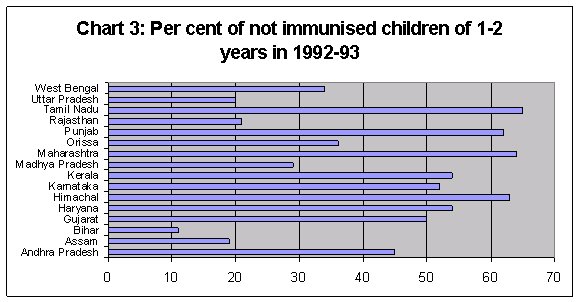
In addition, surveys indicate that even the immunisation services were still well below minimally acceptable norms in the 1990s. Chart 3 shows that most children in the age group 1-2 years were not adequately immunised.
What explains this continuing dismal picture even thirty years after
what is one of the more successful of government schemes was launched
specifically to address these problems? The basic answer must be
that not enough resources have been devoted to this scheme, to meet
the huge requirement. Quite simply, there are not enough anganwadis
or anganwadi workers, and they do not have adequate resources to
meet all the nutritional requirements of those pregnant and lactating
mother, infants and small children who need them. If the declared
norm of one anganwadi per 1000 population is to be met, there should
be 14 lakh anganwadis, as against the current 6.5 lakh such centres,
of which only around 6 lakh centres are operational.
There is the further problem of overloading the tasks assigned to
anganwadi workers. The worker and helper in such centres are paid
so little that they are no more than voluntary workers who receive
a paltry ''honorarium'', and are called ''part-time workers'' in
the centres which are supposed to open for only four hours a day.
Yet they have been found to be among the most dedicated and committed
of public servants who have developed grassroots contacts and are
able to identify particular individuals and groups in any community
easily. They are therefore increasingly engaged in a wide range
of other public interventions, especially in the rural areas.
Some of these other jobs in which the anganwadi workers and helpers
are involved relate to Health Department services such as creating
awareness on diarrhoea and ORS, Upper Respiratory Infections, Directly
Observed Treatment System for Tuberculosis, AIDS awareness, motivation
and education on birth control methods, etc. There are also additional
activities related to the Education Department like Total Literacy
Programmes, Sarva Shiksha Abhiyan, DPEP, Non Formal Education, etc.
In some areas, the close relationship that develops with the local
women makes these women insist that the anganwadi workers accompany
them to the hospital when they go for family planning operations,
their children’s illness, and so on. It is easy to see that all
this amounts to more than a full-time activity, yet the anganwadi
workers and helpers are hardly compensated for all this. In any
case there are simply not enough of them to cater to all of these
varied demands even within a small population.
There are other problems which stem directly from this inadequacy
of centres, staff and resources to run this programme effectively.
It has been found that one of the primary reasons for poor coverage
of needy groups under the scheme is the location of the anganwadi
centre, which typically tends to be in the main village or in upper
or dominant caste hamlets in rural areas in most states. This restricts
the access to such services by deprived communities such as SCs
and STs who live slightly apart. Yet these are precisely the groups
who require it the most.
The expenditure for running the ICDS programme is currently met
from three broad sources:
-
funds provided by the Centre under ‘general ICDS; used to meet expenses on account of infrastructure, salaries and honorarium for ICDS staff, training, basic medical equipment including medicines, play school learning kits, etc.
-
allocations made by the state governments to provide supplementary nutrition to beneficiaries
-
funds provided under the Pradhan Mantri Gramodaya Yojana (PMGY) as additional central assistance, technically to be used to provide monthly take home rations to those children (age group 0 to 3 years) living below the poverty line and in need of additional supplementary nutrition.
There
are frequent complaints of the delay in central government transfer
of resources for this programme, while state governments differ
substantially in the amount and quality of supplementary nutrition
that is provided. This makes the Scheme uneven and sometimes even
problematic in terms of the quality of food provided and its acceptability
to small children.
The original intent of the ICDS programme was to address the various
sub-stages (conception- 1 month, < 3 years and 3-6 years) of
growth in order to ensure that negative health and nutritional outcomes
do not accompany the child from one stage to the next. However,
it has been pointed out by many researchers that the way the programme
has been implemented, it effectively ends up concentrating mainly
on the 3-6 years age group. While children under 3 years are usually
enrolled in the programme, their involvement remains nominal and
there are no facilities to allow for reaching out to such children
and their mothers at home in an effective way.
The timing of the anganwadi centres also effectively rules out many
of the poorest households, since they are open only for four hours
a day. When both parents are working, which is typically the case
among rural labour households in many parts of the country, it is
difficult to deliver and pick up the child from the centre in time,
and so children in such households get excluded from the services.
Once again this really boils down to a question of resources, since
these centres should be open for longer with higher associated expenditure.
These problems have long been recognised, and public interest litigation
(especially by the People’s Union for Civil Liberties, among others)
has ensured that some important orders have been passed by the Supreme
Court in this regard. In 2001, the Supreme Court directed the State
Governments and Union Territories to implement the ICDS in full
and to ensure that every ICDS disbursing centre in the country provide
300 calories and 8-10 grams of protein for each child up to 6 years
of age; 500 calories and 20-25 grams of protein for each adolescent
girl; 500 calories & 20-25 grams of protein for each pregnant
woman and each nursing mother; and 600 calories and 16-20 grams
of protein for each malnourished child. The Court also ordered that
there should be a disbursement centre in every settlement.
Despite this court order, the government was slow to act and very
little was done to ensure that these demands were met even four
years later. However, in the latest Budget Speech of the Finance
Minister, the following promise has been made: ''The universalisation
of the Integrated Child Development Services (ICDS) scheme is overdue.
It is my intention to ensure that, in every settlement, there is
a functional anganwadi that provides full coverage for all children.
As on date there are 6,49,000 anganwadi centres. I propose to expand
the ICDS scheme and create 1,88,168 additional centres that are
required as per the existing population norms. Forty seven per cent
of children in the age group 0-3 are reportedly underweight. Supplementary
nutrition is an integral part of the ICDS scheme. I propose to double
the supplementary nutrition norms and share one-half of the States’
costs for this purpose. I also propose to increase the allocation
for ICDS from Rs.1,623 crore in BE 2004-05 to Rs.3,142 crore in
BE 2005-06.''
This appears very positive, but it is immediately evident that this
is still well below the requirement and that even the additional
centres will still not meet the declared population norms. Quite
clearly, the required expansion, in terms of Central allocation
of resources and hiring of more workers, is much greater than is
being envisaged by the Government even now.
More
significantly, the Finance Minister’s statement can be seen as a
partial attempt to meet the increasing concern of the Supreme Court,
which has already twice reprimanded the government for not doing
enough to ensure the univeralisation and greater effectiveness of
the Scheme. In the latest order, dated 7 October 2004, the Supreme
Court issued very detailed and far-reaching instructions, as follows:
''1. The aspect of sanctioning 14 lakhs AWCs and increase of norm
of rupee one to rupees 2 per child per day would be considered by
this Court after two weeks. (It was subsequently put off following
an affidavit by the Government.)
2. The efforts shall be made that all SC/ST hamlets/habitations
in the country have Anganwadi Centres as early as possible.
3. The contractors shall not be used for supply of nutrition in
Anganwadis and preferably ICDS funds shall be spent by making use
of village communities, self-help groups and Mahila Mandals for
buying of grains and preparation of meals.
4.All State Governments/Union Territories shall put on their website
full data for the ICDS schemes, including where AWCs are operational,
the number of beneficiaries category-wise, the funds allocated and
used and other related matters.
5.All State Governments/Union Territories shall use the Pradhanmantri
Gramodaya Yojna fund (PMGY) in addition to the state allocation
and not as a substitute for state funding.
6.As far as possible, the children under PMGY shall be provided
with good food at the Centre itself.
7.All the State Governments/ Un ion Territories shall allocate funds
for ICDS on the basis of norm of one rupee per child per day, 100
beneficiaries per AWC and 300 days feeding in a year, i.e., on the
same basis on which the Centre makes the allocation.
8.Below Poverty Line shall not be used as an eligibility criterion
for ICDS.
9.All sanctioned projects shall be operationalised and provided
food as per these norms and wherever utensils have not been provided,
the same shall be provided. The vacancies for the operational ICDS
shall be filled forthwith.
10. All the State Governments/Union Territories shall utilise the
entire State and Central allocation under ICDS/PMGY and under no
Circumstances, the same shall be diverted and preferably also not
returned to the Centre and, if returned, a detailed explanation
for non-utilisation shall be filled in the Court.
11.All State/Union Territories shall make earnest efforts to cover
the slums under ICDS.
12.The Central Government and the State/Union Territories shall
ensure that all amounts allocated are sanctioned in time so that
there is no disruption whatsoever in the feeding of Children.''
These are extremely important guidelines, yet it is evident that
the government is not likely to conform to them without sufficient
social and political pressure. It is a sad commentary on the state
of public intervention, that even the most critical schemes that
are universally acknowledged to be necessary to ensure the future
of the country, must be fought for in courts of law and then insisted
upon through activism and people’s struggles.